I’ve found that given time, life does not disappoint in writing material.
I hate this post. I hate writing this post.
Wells was born with an interesting hairline on the back of his head. At twelve months, we took him to get his first haircut and the hairdresser said, “He won’t grow hair there.”

At 18 months old, Wells lost his eyebrows. How does one lose their eyebrows? We chalked it up to KP (Keratosis Pilaris) a skin condition that Wells has and I also have, which can block hair follicles.
Wells wasn’t saying words like the pediatrician’s developmental survey suggested. We brought this up to the doctor and she said, “Let’s give it six months and see what happens.”
Wells’ speech did not improve. He was frustrated when trying to communicate and I contacted a state funded program and got him into speech therapy. Problem solved, right?
We saw the pediatrician six more times within a two month period because of Wells’ eyes. He lost all of his eyelashes. He had a “gunk” that no drops or ointment was alleviating. We were worried about his vision.
The pediatrician told me that she was suspicious that Wells’ medical issues could be linked to a genetic disorder or an auto-immune disease. What? Chris and I didn’t have any genetic markers. We don’t have any auto-immune diseases in our family. I was scared and defensive. She explained that he had many issues; his hair, his skin, his eyes, his developmental delay. Every issue could be a stand-alone problem or it could be tied to something more. She promised she would look into it but in the meantime, she recommended an ophthalmologist to take a look at his eyes.
The ophthalmologist was quick to tell us that Wells’ tear ducts must be blocked in his nasal passageway. His tears were backing up and creating excess mucus in his eyes. She could do a surgical procedure to put in temporary tubes to help his tears drain correctly. We asked her if this issue was linked to any other disorder that she knew of and she said, “Not at all. It’ll be fixed in six months time.” We mentioned Wells’ severe eye sensitivity which she thought was being caused by his many eye treatments. She referred us to an ENT before we scheduled the procedure because of his constant nasal drip.
The ENT saw inflamed nasal passageways. He was confident that Wells’ adenoids needed to be removed. As a last ditch effort to stop the drainage, the ENT prescribed Wells a ten day, antibiotic steroid however, when that didn’t work, we scheduled the adenoidectomy. The ENT also referred Wells to an audiologist after I informed him of Wells’ speech delay. Wells passed the hearing test.
Wells did not want to wear the hospital gown for surgery. The best advice I was given was from my best friend, Lindsey who told me to ask for anxiety medicine for Wells before he went into surgery. Once that was in his system, he was loopy and fine with going back to the surgical room. (I was a crying mess.)
The ENT was able to perform the adenoidectomy while Wells was under the anesthesia from his eye tube surgery. The doctor relayed to us that Wells’ adenoids were enlarged and had pockets of puss; we were glad they were removed. The eye doctor informed us that the eye tubes were inserted perfectly and she was able to fully examine his eyes. She explained to us that Wells had blocked oil glands on his eye lids and because of this, his eyes were not making the correct balance of moisture (water, oil, and mucus). She prescribed a steroidal ointment to try to get the inflammation down on his eyelids so that the oil glands could open.
It was difficult for Wells when he came off the anesthesia. He ripped his IV out and blood got everywhere. He cried for a long time. Once he started drinking, the nurses said we could take him home. I got him a whale balloon from the gift shop that came off it’s string in the parking garage. Chris got on top of the Jeep to rescue it. Wells was happy to eat as much non-dairy ice-cream as he wanted. He had a lot of dried blood on his face the next morning and his breath smelled terrible for a week because of the scabbing.

Six weeks later we went back to the ophthalmologist for a follow up appointment. The ophthalmologist was not thrilled with the results and either were we. Wells’ eyes were still over producing mucus and tears. His eyes were still incredibly sensitive to light. We made an appointment to remove the eye tubes and she referred us to a cornea specialist for further examination.
Our ENT visit was much of the same – disappointing. He still saw significant inflammation in Wells’ nasal passages. He recommended that we see an allergist to rule out environmental allergies for the cause of his inflammation and continued nasal drip.
Our next appointment was with the dermatologist, an appointment that was scheduled six months prior. (Hindsight 20/20 I wish this would’ve been the first appointment we went to.) We spoke to the doctor about Wells’ hair loss. We were very concerned with the condition of his skin. We told her about his recent ENT and eye appointments, as well as his speech delay. The dermatologist was hesitant to say anything definitively but she believed it to be Alopecia Areata, an autoimmune disease that targets inflammation of the hair follicles. She went to get another dermatologist for a second opinion and I cried thinking about the struggles Wells would have to endure.
The next dermatologist was not sold on an Alopecia Areata diagnosis because it would be unusual for the hair loss to start with the eyebrows and eyelashes. She asked us more questions about Wells and his different medical issues when she noticed Wells squinting while looking at my phone screen. She asked, “One final question, does Wells have light sensitivity?” Wells has had severe light sensitivity his entire life. When he is in the sun he must wear a hat and sunglasses or his eyes will roll to the back of his head. His eyes water uncontrollably in bright light. The night before our appointment, Wells complained to us that the TV was too bright. When we told her this information she said, “I have only seen this once, a long time ago during residency, but I think Wells might have a genetic disorder called IFAP.”
The dermatologist was positive that Wells’ issues were being caused by an autoimmune disease or a genetic disorder but she couldn’t be sure which without a blood test. Genetic testing is incredibly expensive so she put in an order through our insurance which took a couple of weeks to get approved. In the meantime, she wanted us to use topical cream for Alopecia just in case that would’ve worked, we would know that the inflammation was caused by the autoimmune disease and we wouldn’t have needed to go through the genetic testing. Not only were these topical meds expensive, I didn’t want to put Wells on any steroids that weren’t absolutely going to solve his problem. Once the order for the blood draw cleared through the insurance, the dermatologist put in an order for the lab to draw blood and check his DNA for two specific compromised genes associated with IFAP syndrome.
Wells’ blood was sent out to a lab in California. The test concluded that his LRP1 gene and MBTPS2 gene were compromised. We were contacted by the dermatologist almost immediately after receiving these results and she confirmed that Wells has the genetic condition, IFAP. IFAP stands for Ichthyosis Follicularis, Alopecia, and Photophobia. IF – his skin, A – his hair loss, and P – his eye sensitivity. This syndrome is a rare X-linked genetic disorder reported in only 40 patients, ever. Don’t Google pictures. My poor baby.
Known to occur in people with IFAP syndrome is corneal abnormalities including a defective tear film and recurrent atopic keratoconjunctival inflammations (exactly what was happening with Wells’ eyes). Did we need to do the tear duct surgery? No. That was never going to fix Wells’ eye issues however, at the time, we were unaware of this genetic disorder. We have since informed the ophthalmologist, who had never heard of IFAP syndrome, of Wells’ diagnosis and she is now researching other cases to better help Wells.

The steroidal cream that Wells was prescribed after his ocular surgery was too strong to be used long term; it could cause too much pressure in the eyes which could lead to glaucoma. We now have to administer an eye drop four times a day and it is not fun, Wells fights us every time. We found out that the drops burn and blur his vision (I contacted the cornea specialist about how it was a terrible experience every time we’d administer his eye drops and she informed us that they are not pleasant but entirely necessary.) It’s been incredibly difficult. He is scheduled to get the eye tubes removed next month as well as a more thorough eye exam by the cornea specialist, all while under anesthesia.
It was time to see the allergist. The ENT wanted to rule out food and environmental allergies for the cause of his nasal drip and inflammation. We explained to the allergist that Wells had been recently diagnosed with IFAP syndrome and that eye and nasal lacrimation are common symptoms of this rare disorder. The doctor called for a full allergy panel, which was administered into Wells’ back. He sat on my lap, facing me, while the nurse pressed the spokes into his skin. He cried and it upset Millie, who came to this appointment. The nurse came back with popsicles for both of them and they were instantly calmed. After ten minutes, the test was complete and Wells showed no signs of allergies. The allergist concluded that any drainage Wells was experiencing was not food or environment related. We were able to rule out allergies and add these drippy symptoms to the list of IFAP complications in Wells’ case.

To better understand IFAP syndrome and what it means for Wells and our family, we saw a geneticist and a genetic counselor. The geneticist was extremely transparent about how fortunate we were to have a doctor (his dermatologist) recognize this syndrome and to “cherry-pick” which chromosomes to test in Wells’ DNA. He told us that there are only 9 recorded cases to have the same mutation as Wells. This syndrome goes undiagnosed because people with these issues do not connect their problems to one diagnosis, and even if they do, they do not know where to begin (the expense of funding a wild-goose-chase of genetic lab work is astronomical). The geneticist believed IFAP to be congenital, meaning the severity of which Wells was born with, will be what he has; for example, he won’t develop mental retardation (a symptom some experience with IFAP). We will see the geneticist yearly to update him on Wells’ developments to hopefully help others learn about this syndrome. He also gave us his card if our new baby is a boy. This way, he can order genetic labs right away.
It was the genetic counselor who explained to us how Wells acquired IFAP syndrome. Males have an X and a Y chromosome, I gave Wells one of my X chromosomes and Chris gave Wells his Y (I couldn’t give Wells a Y chromosome because I don’t have one, I have two X chromosomes because I’m a female). One of my X chromosomes is normal and the other X chromosome is compromised. Because I have one good X, my symptoms of IFAP are lessened therefore, I’m a carrier of the syndrome. Unfortunately, the X that I passed onto Wells was my compromised X chromosome. He doesn’t have another X to combat the compromised X, so his symptoms of IFAP are full force. My father has all of Wells’ same symptoms. His mother, my paternal grandmother, is a carrier. Her father had these same symptoms. The genetic counselor said this is a males syndrome; they give it to their daughters who become carriers, and those daughters give the syndrome to their sons.
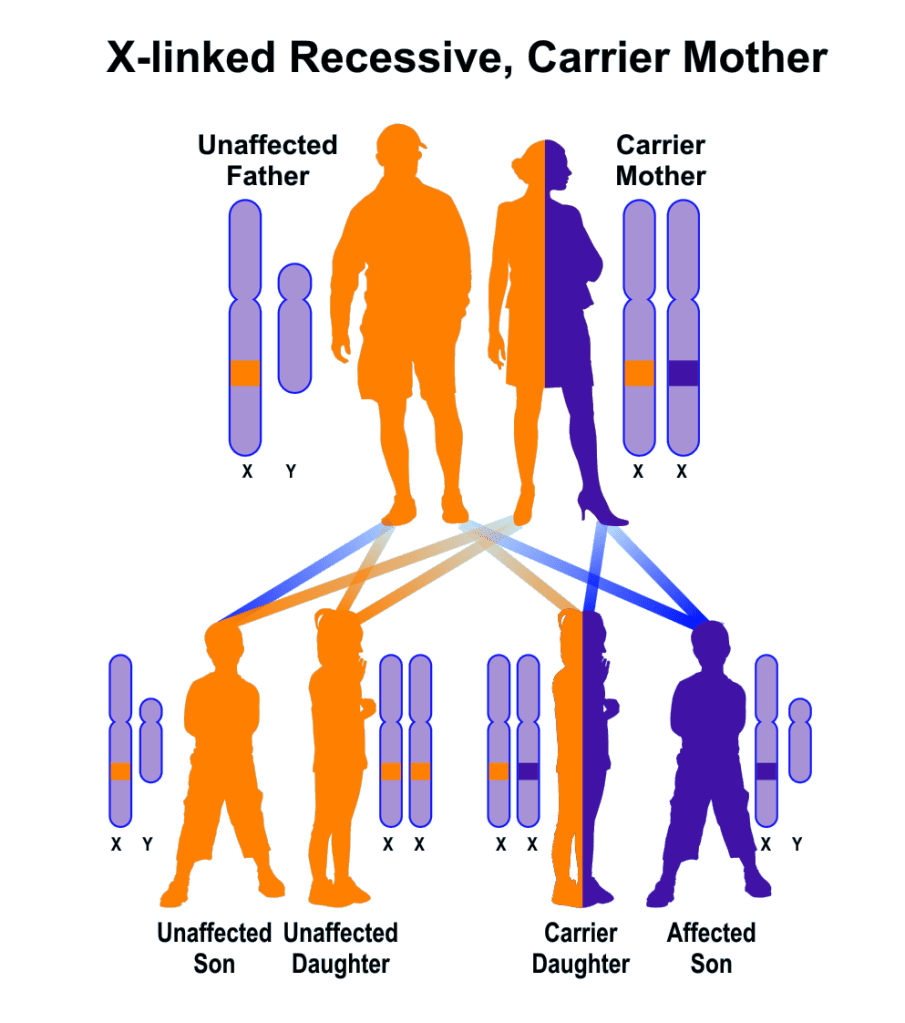
Millie could be a carrier for IFAP syndrome. I could have given her my compromised X but so far, she doesn’t have any IFAP symptoms. She can chose to be genetically tested before she decides to reproduce. If she is a carrier and has a boy, he would have a 50% chance of having IFAP syndrome.
When baby number three is born (we do not know gender) and if the baby is a boy, blood will be drawn while we are in the hospital to be sent to the lab to test for IFAP. At this point, I am hoping that this new baby is a girl OR a boy with my non-compromised X chromosome.
Severe cases of IFAP have noted kidney abnormalities. To make sure Wells’ kidneys developed correctly we took him to get an ultrasound. He was such a brave boy when he was laying on the table. I put my head next to his and we sang Mickey songs together. The tech ran the ultrasound on his belly and his back. She complimented Wells on how well he did and me on my singing. We received the results within the next hour. Wells’ kidneys were sonographically normal and in the normal range for renal dimension. This was a great relief.
In some cases of IFAP, mental retardation is present. With Wells’ CAS (childhood apraxia of speech) diagnosis, we were referred to a neurologist to make sure Wells’ brain was appropriately developed. When we arrived, the nurse gave Wells a sheet of emoji stickers that he stuck to the patient table in a circle and pretended to play duck-duck-goose with them – it was adorable. The neurologist was unfamiliar with IFAP and wanted to test Wells to get a baseline of his development. She asked him questions like, “touch the door, after touching the floor”. She had him stand on one leg. She asked him to point to certain colors, what his best friend’s name was (he said Mia), and to sing his favorite song (the PJ Mask theme song). She was aware of his apraxia and noted that she observed this in his speech however, everything else she tested him on was either developmentally appropriate or advanced for his age. We were thrilled.
The neurologist explained to us that 28-30% of children with IFAP develop seizures. She told us what to look out for if Wells starts to seize and that sometimes seizures don’t look like they do in the movies; he could stare off and not come out of it, one limb could rhythmically move, etc. We have a plan moving forward if he develops this part of the syndrome and until then, Wells does not need to see neurology on a regular basis.
Most recently, we went back to the ENT for the final follow up for Wells’ adenoidectomy. Unfortunately, Wells continues to have a nasal drip. After being tested by the allergist at the ENT’s request, we found that Wells has no allergies alas, his nasal drip is not caused by allergies. The doctor checked to make sure Wells hadn’t put anything up his nose (he did not). He checked his ears and throat (both of which looked great). It was determined that Wells’ drainage is IFAP related but to what extent, the ENT wasn’t sure. While he discusses the possibilities of why this is happening with the geneticist, he put Wells on a steroidal nasal spray to reduce his inflammation. The ENT believes this will be a chronic issue for Wells.
Through the Ohio Department of Health we are in the process of applying for CMH which stands for Children with Medical Handicaps. This health care program will help to offset the costs of Wells’ medical needs.
This diagnosis is beyond scary. All I want to do is help my baby and take this away for him. Unbeknownst to me, I was the one to give this to him. There is a perpetual feeling of guilt that I have to suppress as I need to focus on what Wells is going through and his needs. I will forever be his advocate as we navigate this syndrome, together.
